Simple’s guide on intermittent fasting and cholesterol

Cholesterol is a substance that our body makes naturally. We need some of it for good health and function. But when it gets out of whack, it puts us at risk of health problems. Almost 2 in 5 adults in the United States have high cholesterol, and high cholesterol doesn’t have any symptoms.[1]
So, how can we help lower our risk? Does intermittent fasting lower cholesterol, and can it be part of our heart-healthy lifestyle?
In this article, we’ll explore the link between fasting and cholesterol, explain what may improve our cholesterol profile, and share tips to help you lower your risk.
Ready to take control of your cholesterol levels? Uncover personalized insights by taking the Simple quiz now. Find out how intermittent fasting, coupled with our in-app features, can be your secret sauce for a healthier heart!
What is cholesterol, and how does it work?
Cholesterol is a waxy, fat-like molecule.[2] While it’s gotten a bad rap recently, we actually need cholesterol for key physiological processes and overall good health.[3]
For example:[2]
- Cholesterol helps form cell membranes, the fluid “envelopes” around every cell in the body, and affects how permeable those membranes are (which then affects what substances can get in and out of cells).
- Cholesterol also helps produce essential compounds like vitamin D, steroid hormones like cortisol, and sex hormones like estrogen and testosterone.
- Cholesterol helps us digest and absorb the important fat-soluble vitamins A, D, E, and K.
While we often think of cholesterol as being in high-fat foods like bacon or egg yolks, most of our circulating cholesterol is made in our own bodies.
While all cells can synthesize (or make) at least a little cholesterol to a small extent, our liver makes most of our cholesterol as part of its normal job.[4]
In the liver, cholesterol is transformed into bile acids, which are important in digestion. (If you’ve ever had a gallbladder issue, you know what happens when this goes wrong.) When bile acids are released from the gallbladder into the small intestine, they mix with the cholesterol in the foods we may have eaten.
Some of the cholesterol is reabsorbed, while the rest leaves the body in feces (aka poop) — which is one reason why a high-fiber diet is important for managing cholesterol levels, as fiber can bind to cholesterol and help it leave the body.
So, we’re always releasing and absorbing cholesterol, losing about 2% of it per day (or around 1 to 2 grams).[4,5]
To make this all work, our body needs a way to transport cholesterol around. And that’s when we get to different cholesterol types.
Types of cholesterol
Because cholesterol is fat-based, it doesn’t mix well with water-based blood. So, cholesterol — as well as other fatty substances, like triglycerides — needs the help of lipoproteins to get around the body.[6] These are sort of like little inner tubes that cholesterol can hitch a ride on through the bloodstream.
(“Lipo” means fat-based — think “liposuction” — and “protein” means, well, protein. Lipoproteins are able to hang on to fats, aka lipids, while traveling through water-based blood like a protein.)
Much of the “cholesterol test” or lipid profile blood test you’d do with your doctor actually involves testing levels of these lipoproteins and triglycerides, not just cholesterol levels alone.
There are different types of lipoproteins with different sizes and densities. These differences also define how they act in our bodies since they actually carry the same type of cholesterol.[4–6]
Two of the key players include:
- High-density lipoprotein (HDL) is often called “good” cholesterol. Its job is to take cholesterol from cells back to the liver. As its name suggests, high-density lipoprotein particles are small and dense. Think of them as little recycling trucks bringing cholesterol back to the depot.
- Low-density lipoprotein (LDL) is often referred to as “bad” cholesterol. Its job is to move cholesterol from the liver or intestines to cells that then use the cholesterol for various jobs. While we need LDL, when it’s too high, it can cause problems.[6]
However, there are many other types of lipoproteins.
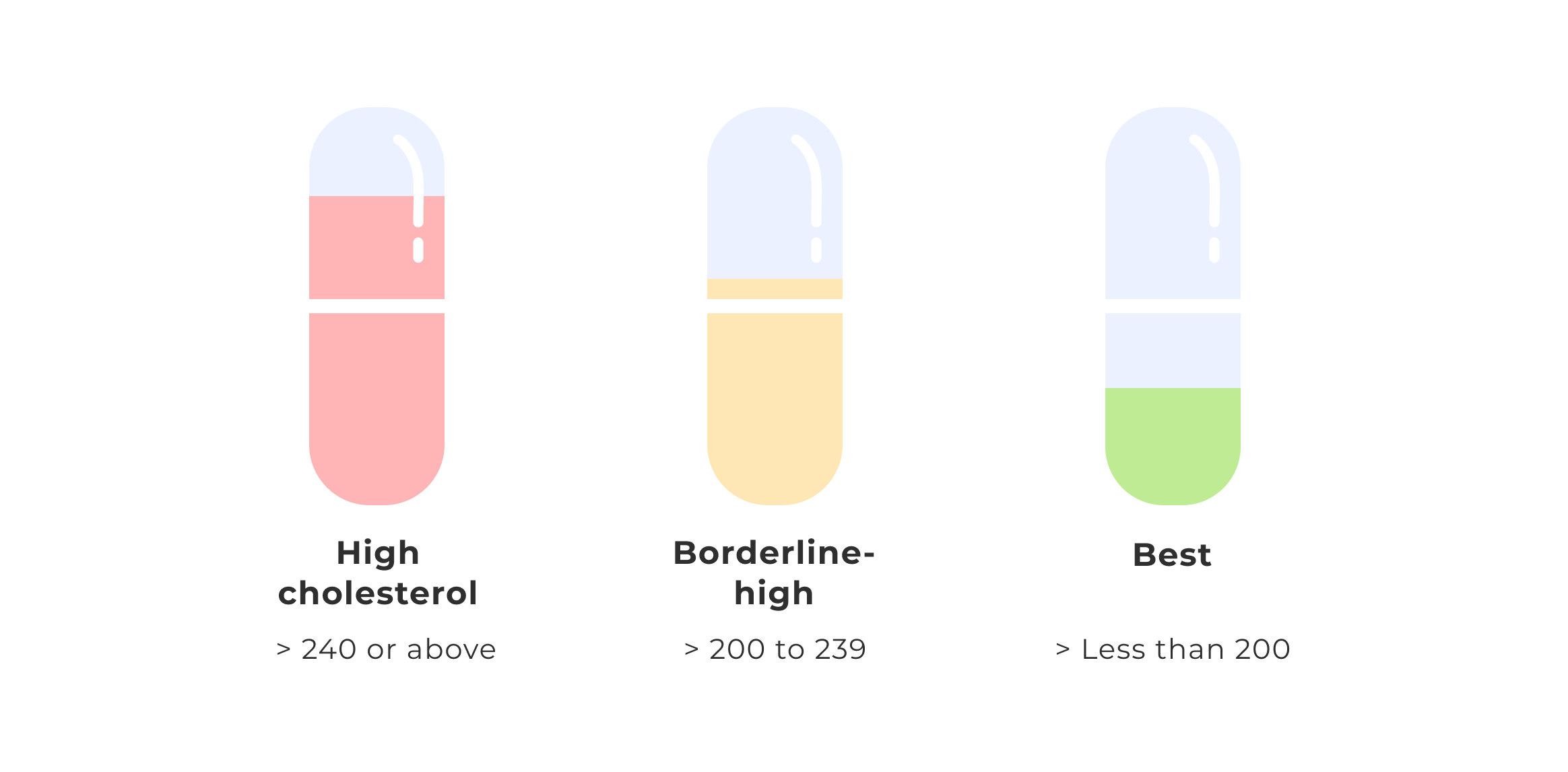
When you do a basic “cholesterol test” with your doctor, this blood test will likely look at:
- total cholesterol
- triglycerides (fats in your bloodstream)
- HDL (sometimes called HDL-C for cholesterol)
- LDL (sometimes called LDL-C)
The levels of all of these can help your doctor assess your risk of heart disease.
Looking to improve your overall health so that those tests come back with the results you want? Jump into the Simple quiz and explore how intermittent fasting, along with our smart food tracker and hydration helper, can transform your wellness journey. Take the first step to a heart-healthy lifestyle!
Does intermittent fasting impact cholesterol levels?

While it might seem like eating a lot of cholesterol would always result in high circulating cholesterol, it doesn’t always work that way. Normally, around 25%–30% of our body’s cholesterol comes from our diet.[7] Our body’s own cholesterol-making system adapts to how much cholesterol we eat.[8]
But what about if we’re not eating, as is the case with intermittent fasting? By ensuring we have periods when we aren’t eating anything, can fasting lower cholesterol?
Potentially yes. When fasting, we mainly use stored body fat for energy, turning fats into ketones that our cells can use. Some research suggests that this process in the liver can switch on certain genes that then affect not just fat burning but cholesterol levels, too.[9]
One systematic review explored whether intermittent fasting could lower cholesterol and affect other cardiometabolic risk factors. They checked various scientific databases for studies comparing intermittent fasting to other diets.[9]
The results showed that compared to the control group, people on intermittent fasting reduced their
- body weight
- waist circumference
- body fat
- BMI
- blood pressure
- total cholesterol
- triglycerides
- fasting insulin
- insulin resistance
However, no significant differences were found for the “bad” low-density lipoprotein cholesterol (LDL), the “good” high-density lipoprotein cholesterol (HDL), or A1c glycosylated hemoglobin (a marker that measures how well someone can control their blood sugar).[10]
Another similar large study looking at possible links between intermittent fasting and cholesterol found that intermittent fasting did significantly change total cholesterol levels. And intermittent fasting did seem to be able to decrease high LDL cholesterol along with triglycerides. But there was no notable change in the “good” HDL cholesterol.[11]
That said, some other smaller studies have found that HDL increased with intermittent fasting.[12,13] Why does fasting increase this type of cholesterol? We still aren’t sure, and we need more research to understand this connection.
So, does fasting affect cholesterol? Can intermittent fasting lower cholesterol, if that’s a concern?
It seems the answer is: it depends.
Most studies on intermittent fasting do suggest that fasting lowers the risk of cardiovascular disease markers that include cholesterol.
For instance, another review of several intermittent fasting studies suggests that for people who practice fasting:[14]
- Total cholesterol typically goes down by 6% to 21%.
- LDL cholesterol goes down by 7% to 32%.
- Triglyceride levels go down by 16% to 42%.
- Plus, systolic and diastolic blood pressure go down by 3% to 8% and 6% to 10%, respectively.
While some of these benefits might come from weight loss, there may be other mechanisms at work. For instance, managing blood sugar and achieving a healthy body weight can also play a role.
Obesity is linked to dyslipidemia — having a higher-risk lipid profile that may predispose people to cardiovascular diseases.[15]
The same is true in type 2 diabetes.[16] Poor glycemic control (i.e., not controlling blood glucose levels properly) in type 2 diabetes increases triglyceride, raises “bad” LDL, and decreases “good” HDL-C levels.[16] Intermittent fasting may be helpful for diabetes, and unlike cholesterol, the evidence here is more clear.
Although the results are promising, we still need more research to answer questions like “Does intermittent fasting lower cholesterol, and if so, how can we ensure it works the way we want?” For instance, if it turns out that intermittent fasting raises HDL cholesterol, is that a good thing? Stay tuned!
Who should avoid intermittent fasting?
Intermittent fasting is safe for beginners and experienced fasters alike. While intermittent fasting does have a few side effects, most healthy adults will do fine with fasting, no matter what their body type. This is especially true if they’re careful to avoid some common intermittent fasting mistakes.
However, fasting is NOT a good option for folks who:
- are pregnant or breastfeeding
- are younger than 18 or 80 years old or more
- have been diagnosed with an eating disorder or have a history of one
- have a medical condition (or are taking medications) that makes fasting unsafe
- need a lot of calories every day (such as elite athletes doing hours of exercise)
When to consult a doctor
Consulting a doctor is a great idea if you’re considering intermittent fasting and/or worried about your cholesterol levels. While intermittent fasting is safe for most healthy adults, there may be other health concerns in the mix that you should discuss with a healthcare provider.
If you’re 40 or older, it’s wise to schedule regular checkups that include both blood sugar management tests (such as fasting insulin levels) and blood lipid tests.
(BTW, if you’ve gotten the okay from your healthcare provider to start fasting, tag us in, and we’ll support you on your intermittent fasting journey. Take our Simple quiz to get started today!)
Simple’s tips on controlling cholesterol levels with intermittent fasting

Does fasting reduce cholesterol? The answer depends on each individual and which type of cholesterol.
That said, here are some handy tips to get the most out of your intermittent fasting journey:
- Combining intermittent fasting with good nutrition (and lower calories, if appropriate) likely works better than fasting alone.[11] Although what to eat during intermittent fasting is flexible, it’s still a wise idea to ensure you’re eating nourishing, nutrient-dense foods when you do eat.
- It might sometimes look like intermittent fasting is not working, but this likely means you need to make some small adjustments. By using Simple’s food, activity, and hydration trackers, you can help yourself pinpoint where you might make changes to get the results you want.
- Regular exercise also appears to improve cholesterol levels.[17,18] For instance, being consistently active lowers triglycerides and “bad” LDL levels while increasing “good” HDL levels. So, combining intermittent fasting, a healthy diet, and regular exercise can be a threefold boost to your cardiovascular health!

Frequently asked questions about intermittent fasting and cholesterol
Most often, no. While some smaller studies have found that longer-duration fasting (think 7 days) does increase LDL cholesterol and triglycerides [21] (likely because people are now using stored body fat exclusively for energy at that point), this doesn’t really apply to most regular people doing time-restricted eating (TRE) of 16 hours or less. (And we definitely don’t recommend that type of fasting unless you’re being closely medically supervised.)
But in general, regular intermittent fasting seems to lower LDL or have no effect.
While black coffee is on the list of what you can drink while fasting, some evidence suggests that in some people, coffee may raise cholesterol levels.[22,23]]
This is likely related to additional ingredients added to coffee, such as milk or flavored syrups, and maybe accompanying snacks, as opposed to the coffee bean itself. We suggest limiting coffee consumption to less than 3 a day, and consult with your healthcare provider if you have any concerns.[24]
The relationship between mood disorders like anxiety and depression and cholesterol is mixed.[26]
Some suggest that when cortisol goes up during chronic stress, it may change cholesterol levels. Others suggest that because of cholesterol’s role in cell membranes (and sending signals in the brain), disrupted cholesterol levels may come first and contribute to mood issues.
If you have concerns about your mental and emotional health or your cholesterol levels, make sure to consult with your doctor.
- CDC. Cholesterol [Internet]. Centers for Disease Control and Prevention. 2023 [cited 2023 Nov 9].
- Craig M, Yarrarapu SNS, Dimri M. Biochemistry, Cholesterol. StatPearls Publishing; 2023.
- Huff T, Boyd B, Jialal I. Physiology, Cholesterol. StatPearls Publishing; 2023.
- Saher G. Cholesterol Metabolism in Aging and Age-Related Disorders. Annu Rev Neurosci. 2023 Jul 10;46:59–78.
- Feingold KR. Introduction to Lipids and Lipoproteins. MDText.com, Inc.; 2021.
- Lent-Schochet D, Jialal I. Biochemistry, Lipoprotein Metabolism. StatPearls Publishing; 2023.
- Blesso CN, Fernandez ML. Dietary Cholesterol, Serum Lipids, and Heart Disease: Are Eggs Working for or Against You? Nutrients [Internet]. 2018 Mar 29;10(4).
- Röhrl C, Stangl H. Cholesterol metabolism-physiological regulation and pathophysiological deregulation by the endoplasmic reticulum. Wien Med Wochenschr. 2018 Sep;168(11-12):280–5.
- Malinowski B, Zalewska K, Węsierska A, Sokołowska MM, Socha M, Liczner G, et al. Intermittent Fasting in Cardiovascular Disorders—An Overview. Nutrients. 2019 Mar 20;11(3):673.
- Eyth E, Naik R. Hemoglobin A1C. StatPearls Publishing; 2023.
- Meng H, Zhu L, Kord-Varkaneh H, O Santos H, Tinsley GM, Fu P. Effects of intermittent fasting and energy-restricted diets on lipid profile: A systematic review and meta-analysis. Nutrition. 2020 Sep;77:110801.
- Ahmed N, Farooq J, Siddiqi HS, Meo SA, Kulsoom B, Laghari AH, et al. Impact of Intermittent Fasting on Lipid Profile-A Quasi-Randomized Clinical Trial. Front Nutr. 2020;7:596787.
- Kelly CJ. A controlled trial of reduced meal frequency without caloric restriction in healthy, normal-weight, middle-aged adults. Am J Clin Nutr. 2007 Oct;86(4):1254–5.
- Anton SD, Moehl K, Donahoo WT, Marosi K, Lee SA, Mainous AG 3rd, et al. Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting. Obesity . 2018 Feb;26(2):254–68.
- Vekic J, Stefanovic A, Zeljkovic A. Obesity and Dyslipidemia: A Review of Current Evidence. Curr Obes Rep. 2023 Sep;12(3):207–22.
- Feingold KR, Grunfeld C. Diabetes and Dyslipidemia. In: Johnstone M, Veves A, editors. Diabetes and Cardiovascular Disease. Cham: Springer International Publishing; 2023. p. 425–72.
- Muscella A, Stefàno E, Marsigliante S. The effects of exercise training on lipid metabolism and coronary heart disease. Am J Physiol Heart Circ Physiol. 2020 Jul 1;319(1):H76–88.
- Doewes RI, Gharibian G, Zadeh FA, Zaman BA, Vahdat S, Akhavan-Sigari R. An Updated Systematic Review on the Effects of Aerobic Exercise on Human Blood Lipid Profile. Curr Probl Cardiol. 2023 May;48(5):101108.
- Blood Cholesterol: Causes and Risk Factors [Internet]. NHLBI, NIH. [cited 2023 Nov 24].
- Kanter MM, Kris-Etherton PM, Fernandez ML, Vickers KC, Katz DL. Exploring the factors that affect blood cholesterol and heart disease risk: is dietary cholesterol as bad for you as history leads us to believe? Adv Nutr. 2012 Sep 1;3(5):711–7.
- Sävendahl L, Underwood LE. Fasting increases serum total cholesterol, LDL cholesterol and apolipoprotein B in healthy, nonobese humans. J Nutr. 1999 Nov;129(11):2005–8.
- De Roos B, Van Tol A, Urgert R, Scheek LM, Van Gent T, Buytenhek R, et al. Consumption of French-press coffee raises cholesteryl ester transfer protein activity levels before LDL cholesterol in normolipidaemic subjects. J Intern Med. 2000 Sep;248(3):211–6.
- Ren Y, Wang C, Xu J, Wang S. Cafestol and Kahweol: A Review on Their Bioactivities and Pharmacological Properties. Int J Mol Sci [Internet]. 2019 Aug 30;20(17).
- Du Y, Lv Y, Zha W, Hong X, Luo Q. Effect of coffee consumption on dyslipidemia: A meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2020 Nov 27;30(12):2159–70.
- Patikorn C, Roubal K, Veettil SK, Chandran V, Pham T, Lee YY, et al. Intermittent Fasting and Obesity-Related Health Outcomes: An Umbrella Review of Meta-analyses of Randomized Clinical Trials. JAMA Netw Open. 2021 Dec 1;4(12):e2139558.
- Papakostas GI, Ongür D, Iosifescu DV, Mischoulon D, Fava M. Cholesterol in mood and anxiety disorders: review of the literature and new hypotheses. Eur Neuropsychopharmacol. 2004 Mar;14(2):135–42.